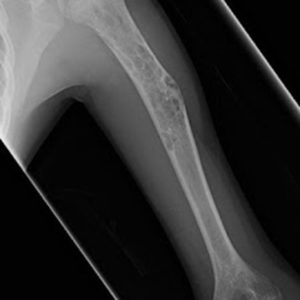
A historical asymptomatic population revealed an 18.9% prevalence of benign childhood bone tumors of the extremities, according to results. Christopher D.…
Rapamycin impairs mitochondrial function in guinea pig model By Federation of American Societies for Experimental Biology (FASEB) New research presented virtually…
Coronavirus disease 2019 (COVID-19) is an emerging pandemic disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Epidemiological…
A single, multidisciplinary session of an individual intervention combining detailed information on functioning, activities of daily living, physical activity, nutrition,…
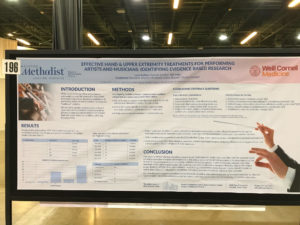
Dr. Collins discusses his latest research study, “Effective Hand & Upper Extremity Treatments for Performing Artists and Musicians: Identifying Evidence…